“The news that could kill me arrived on my phone like a weather alert.”
The Diagnosis – Coronary Artery Disease
The news didn’t come from a cardiologist’s voice, weighted with gravitas, but from a push notification on the Kelsey-Seybold app. A note from a physician assistant. CAD-RADS 2: Coronary Artery Disease, 25–49% narrowing in at least one coronary artery. Ninety-nine percent of men my age, it said, show less calcium deposits in their heart than I do. The angina I had half-convinced myself was imaginary had been real all along. And the message was blunt enough to pierce even my well-practiced rationalizations. I was advised to either get my lifestyle in order, or get my affairs in order.
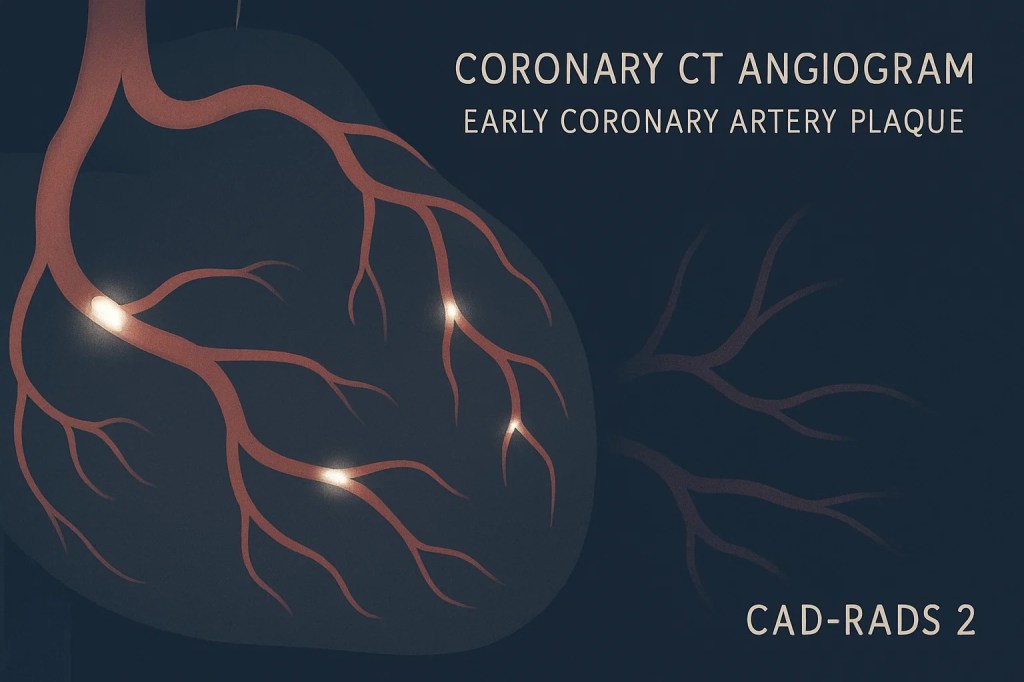
That line landed with more force than the number itself. CAD-RADS 2 isn’t an emergency, but it isn’t benign. It’s the quiet stage of the disease where the soft plaques lining my heart arteries are poised to break loose and turn into something catastrophic. The ECG had shown nothing, no Q-waves from previous heart attacks, and the treadmill stress test had shown nothing. My cardiologist told me before the diagnosis, “you seem stubborn”, and I felt healthy enough to dismiss the little warning signs. But chest pain “at my age” should be taken seriously. He ordered the half-day long CT Angio scan with contrast to reveal the truth hiding under the appearance of fitness.
Because I did not look like a failing body. (I had just finished a half-marathon in the mountains a month before!) And with a history of competitive sports and triathlons stretching back years, I convinced myself I was doing just fine. My Garmin smart watch, my data logs, my identity all said, “fit and in fighting form”. But my arteries now revealed otherwise. I could no longer outrun the diagnosis; in fact, running hard was part of the current problem! With the chest tightness and this diagnosis, I was relegated to keeping my heart rate under 152 bpm, only modestly into my full range between a RHR of 45 bpm and MaxHR of 189, staying in the safe zone while the medicine and lifestyle changes did their slow work of hardening the plaques, armoring them so they wouldn’t rupture.
What made the moment uncanny wasn’t just the medical result but the realization that the old calculus, fitness equals health, had collapsed. I was fit, but failing. And the ledger that had been hidden was suddenly made visible: sugar, stress, and skepticism, each leaving its signature on the CT scan.
The Ledger of Sugar
Sugar was my first and most persistent addiction, though I never thought to call it that. It threaded through everything: the spoonfuls stirred into coffee, the quiet tins of candy on every trading floor, the ritual bowl of cereal that ended most nights. I never went more than a handful of hours without something sugary & refined. Hunger wasn’t the driver, craving was, and only something sweet could quiet the want.
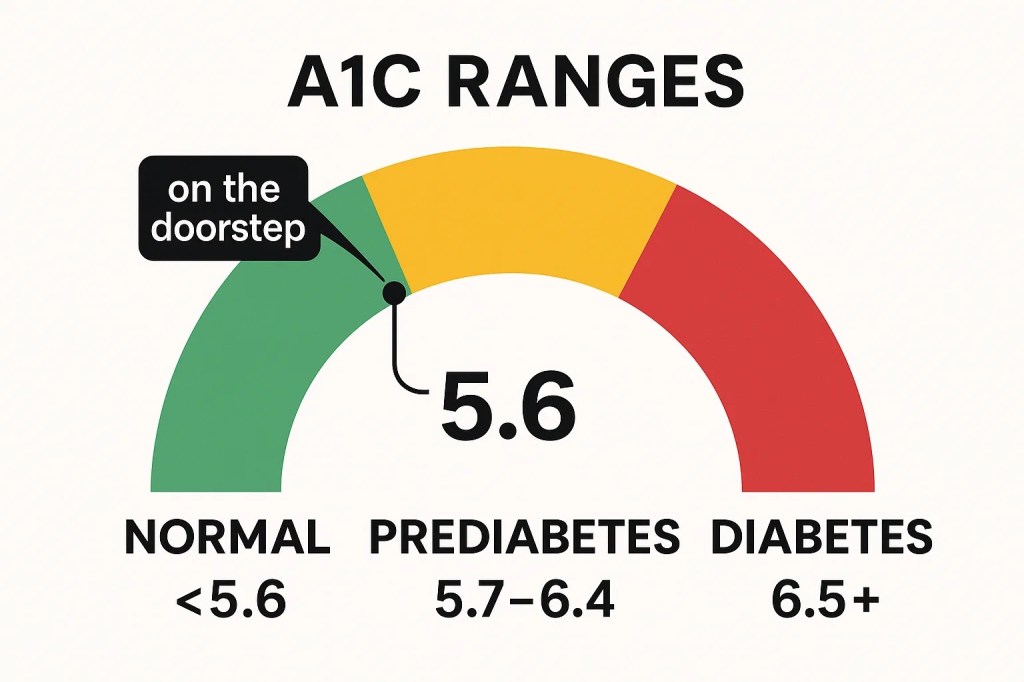
The labs had been warning me long before the scan did. Year after year they showed a drift away from insulin sensitivity and toward insulin resistance, the quiet slope toward diabetes. Just before the CAD-RADS 2 diagnosis, my A1C came back at 5.6, a tenth of a point shy of the diabetic threshold. I was standing at the doorstep.
Most people wouldn’t have called me overweight. At six foot two inches, I carried 225 pounds without looking soft, a frame that once fit both rugby and competitive swimming, and later put me in the Clydesdale category of runners. (In marathons and 70+ mile triathlons I wasn’t fast, but I liked to call myself “unkillable”, the sort who could grind for hours and hours without quitting.)
I wore endurance like armor, and endurance let me hide.
I told myself I could run it off, that the miles burned through the excess. But the body doesn’t reconcile the ledger that way. Glycogen stores that were never depleted, a liver pushed to constant overdrive, the “math didn’t math”, as we sometimes joke on trading floors. My watch metrics looked fine; my actual blood metrics did not. And I ignored the data that didn’t match up with my high opinions of my fitness.
What I see now is that sugar wasn’t a harmless indulgence or a quirk of taste but a smoking gun. Every spoonful layered itself, slowly and invisibly, into the calcification of my arteries. Because I looked like an athlete, I thought I was immune. But the scan proved otherwise: sugar is the enemy you don’t see, until suddenly you can.
The Baseline of Stress
If sugar was the first driver of my diagnosis, stress was the constant hum in the background, the baseline I mistook for silence. Decades of Front Line Energy Commodity Trading as a career does that. The “wake and work” cadence of international markets, screens lighting up before dawn, cortisol pegged high by 6 a.m., and carried like a full ruck-sack through to the evening. Add to that the rituals of the energy trading business itself: dinners, drinks, the alcohol-as-lubricant of trading relationships. It wasn’t just a job, it was a three decade physiology.
My solution was fitness. Always fitness. Long runs, endless bike miles, hours in the pool, all justified as “stress relief.” But exercise is not the same thing as absence of stress; it is only another form of stress. What I learned, but not for many years, was how to put the phone down, how to carve out the true space where cortisol could ebb. From pagers and payphones in the 1990s to BlackBerry’s in the 2000s to the current smartphone era that dissolved any boundary between work and life, I lived plugged in. It is a point of pride among traders, and it was (is) slowly killing some of us. Mornings, evenings, weekends. An off-switch was for other roles.
Looking back, before 2020, I could not recall a single uninterrupted week away from my device, not one. Stress was not episodic for me; it was the medium I breathed in. And cortisol, when it isn’t discharged, does not vanish, it builds. It rides along the dopamine gradient, it spikes with fear, it keeps the body in a constant state of alert, fight-or-flight humming in the background even during supposed rest.
Only recently have I begun to test other responses. meditation, genuine technology breaks, the act of stillness itself. But the ledger is already visible. A CT scan of my arteries looks less like an anatomy lesson and more like reconnaissance photography of a bombed-out city. Stress carved its own architecture into me, and the proof is etched in calcium. This was not an acute result, this was the outcome of chronic and decades of choices.
When Skepticism Calcifies
Skepticism has always been part of my worldview. It’s how I navigate markets, institutions, every relationship, I assume all claims are provisional, test them, verify or discard. But skepticism can calcify. When it hardens, it stops being a method and starts looking like a belief system. And belief, when it is wrong, locks you out of progress.
I was skeptical of statins for years, and not without reason. The first generation, the lipophilic statins, were implicated in cognitive side effects, memory lapses, that foggy sense of diminished sharpness. Modestly, after my dashing good looks, my brain is the next most valuable part of my personal brand, and I wasn’t about to gamble with it. I was also skeptical of the LDL narrative itself. If I had a genetic predisposition to carry higher LDL, maybe (I thought) it was evolutionary ballast; a gift to help my ancestors through lean times. But I have never experienced lean times. In the modern Standard American Diet (SAD), excess LDL oxidizes into VLDL, raises ApoB, and quietly vandalizes arterial walls.
My skepticism wasn’t purely intellectual; it was emotional. Anything called a “statin” sounded blunt, industrial, a hammer where I wanted a scalpel; a personal solution based on hard work and discipline, not a pill. Aside from a few antibiotics, I’d never had a prescriptions that lasted more than a month. So I delayed. I convinced myself I had time. And in that delay, the damage accumulated, invisible but measurable, until the CT scan spelled it out.
Only then did I return to the research with fresh urgency. What I found was that medicine had not stood still while I was hesitating. Hydrophilic statins had emerged, rosuvastatin, designed to bypass many of the cognitive side effects I feared. And the new evidence showed more than LDL reduction. These drugs not only slow the conversion of LDL into oxidized particles, they reduce vascular inflammation itself, giving arteries the break they need to stabilize.
So now I take 20 mg of rosuvastatin each night, a 90-day initiation alongside dietary and lifestyle changes. Skepticism is still in me, it will always be there, honed by years of bad advice swinging from margarine to butter, eggs bad to eggs good, fat condemned then redeemed. The health sciences have their fads. But this time I’ve chosen not to let doubt calcify. Skepticism should be a tool for progress, not a barricade against it.
The Science
The three culprits I’ve laid out; sugar, stress, and skepticism are grounded in the current medical literature. The science is unambiguous that these factors converge on the arteries.
At a population level, excess sugar consumption drives insulin resistance, elevated triglycerides, and eventually prediabetes. Even at levels shy of diabetes (A1C of 5.6–5.7), studies show a measurable increase in coronary plaque and calcium on CT scans [1][2]. In other words, the slow slide from insulin sensitivity to resistance is not benign, it leaves its mark on the vascular wall. “Sugar was here!”
Chronic stress carries its own signature. Sustained cortisol elevation alters blood pressure, glucose metabolism, and lipids, while also feeding inflammatory pathways that damage the endothelium [3][4]. Longitudinal studies confirm that people with persistently high stress hormone levels develop hypertension and suffer more heart attacks and strokes over time[5]. Stress is not just a mental burden; it is a structural risk factor for atherosclerosis.
Finally, skepticism. Early concerns about lipophilic statins and cognitive decline never held up under controlled trials[6]. Newer hydrophilic statins like rosuvastatin show no cognitive harm, and in some data even correlate with reduced dementia risk[7]. The broader consensus is that lowering LDL and, more importantly, total ApoB-containing particles (LDL, VLDL, remnants, Lp(a)) is central to reducing cardiovascular events[8]. High LDL, whether genetic or acquired, contributes to atherosclerosis over time, the data supports that excess LDL is not simply neutral ballast.
Taken together, the evidence reinforces the diagnosis: sugar fuels the metabolic fire, stress fans it, and skepticism delayed the intervention that could have dampened it.
Resolutions
Immediate Actions (the first 90 days)
I have already begun the first line of defense: rosuvastatin 20 mg nightly, not as concession but as tool, to quiet vascular inflammation and slow the chemistry of plaque rupture. I will pair this with disciplined nutrition, fasting through the day when possible, eating in an 18-6 intermittent fasting protocol, evening meals weighted toward vegetables, legumes, and fish, away from sugar and refined starch. My A1C of 5.6 leaves no margin for denial; glycemic control is no longer optional. Fitness & training will remain daily but within safe zones: heart rate capped below 152 bpm, most HR2 miles and ample swimming of laps, all volume laid down in the aerobic band. Each week I will log blood pressure, body weight, and sleep, not as vanity metrics but as signals to watch and to trend. I will repeat lipid panels and liver enzymes after 90 days, a check against both the medicine and my resolve to improve my lifestyle.
Medium-Term Practices (6–12 months)
The next horizon is adaptation. To turn daily intermittent fasting and quarterly 96-hour fasts into rhythm rather than ordeal. To carry a Mediterranean Diet pattern forward: whole grains sparingly, extra-virgin olive oil as staple, alcohol as a rare exception. Vitamin D repletion has already lifted me from deficiency; I will maintain it. Strength work will cycle heavy to light, glute and posterior chain emphasized, not to sculpt but to offload strain from heart and joints. Stress practice must become deliberate: meaningful meditation, walks without my phone, evenings with no glow of screens. I will trial full weeks off technology, an act I once thought impossible. At each turn the proof will not be in feeling but in data, lipids bending down, kidney function stable, liver enzymes clear.
Long-Term Commitments (multi-year)
Over years, the project is not to outpace disease but to deny it momentum. To keep LDL in a useful range and arterial plaques armored, not softened and unstable. To make endurance serve health, not ego. To treat stress as hazard, not habit. To maintain skepticism as an instrument but refuse its calcification into paralysis. My aim is not purity, nor immortality, but the simplest of metrics: arteries that remain open, blood that continues to flow, my allotment of days long enough for work worth doing.
I do not mistake this for victory. It is maintenance, vigilance, the discipline of living within limits without being reduced by them. Sugar, stress, and skepticism each took their turn at the ledger. Now the balance is mine to write, and the pen rests in my hand.
End Notes
On Sugar …
[1] Overgaard, K. S., Andersen, T. R., Mohamed, R. A., Heinsen, L. J., Binderup, H. G., Möller, S., Auscher, S., Lambrechtsen, J., & Egstrup, K. (2023). Can prediabetes diagnosed using HemoglobinA1c or oral glucose tolerance test predict presence and severity of coronary artery disease in symptomatic patients?. Diabetes & vascular disease research, 20(3), 14791641231179870. https://doi.org/10.1177/14791641231179870
[2] Huang, Y., Chen, Z., Chen, B., Li, J., Yuan, X., Li, J., Wang, W., Dai, T., Chen, H., Wang, Y., Wang, R., Wang, P., Guo, J., Dong, Q., Liu, C., Wei, Q., Cao, D., & Liu, L. (2023). Dietary sugar consumption and health: umbrella review. BMJ (Clinical research ed.), 381, e071609. https://doi.org/10.1136/bmj-2022-071609
On Stress …
[3] Osborne, M. T., Shin, L. M., Mehta, N. N., Pitman, R. K., Fayad, Z. A., & Tawakol, A. (2020). Disentangling the Links Between Psychosocial Stress and Cardiovascular Disease. Circulation. Cardiovascular imaging, 13(8), e010931. https://doi.org/10.1161/CIRCIMAGING.120.010931
[4] Gu, H. F., Tang, C. K., & Yang, Y. Z. (2012). Psychological stress, immune response, and atherosclerosis. Atherosclerosis, 223(1), 69–77. https://doi.org/10.1016/j.atherosclerosis.2012.01.021
[5] Inoue, K., Horwich, T., Bhatnagar, R., Bhatt, K., Goldwater, D., Seeman, T., & Watson, K. E. (2021). Urinary Stress Hormones, Hypertension, and Cardiovascular Events: The Multi-Ethnic Study of Atherosclerosis. Hypertension (Dallas, Tex. : 1979), 78(5), 1640–1647. https://doi.org/10.1161/HYPERTENSIONAHA.121.17618
On Skepticism & Statins …
[6] Zhou, Z., Ryan, J., Ernst, M. E., Zoungas, S., Tonkin, A. M., Woods, R. L., McNeil, J. J., Reid, C. M., Curtis, A. J., Wolfe, R., Wrigglesworth, J., Shah, R. C., Storey, E., Murray, A., Orchard, S. G., Nelson, M. R., & ASPREE Investigator Group (2021). Effect of Statin Therapy on Cognitive Decline and Incident Dementia in Older Adults. Journal of the American College of Cardiology, 77(25), 3145–3156. https://doi.org/10.1016/j.jacc.2021.04.075
[7] Ott, B. R., Daiello, L. A., Dahabreh, I. J., Springate, B. A., Bixby, K., Murali, M., & Trikalinos, T. A. (2015). Do statins impair cognition? A systematic review and meta-analysis of randomized controlled trials. Journal of general internal medicine, 30(3), 348–358. https://doi.org/10.1007/s11606-014-3115-3
[8] Soffer, D. E., Marston, N. A., Maki, K. C., Jacobson, T. A., Bittner, V. A., Peña, J. M., Thanassoulis, G., Martin, S. S., Kirkpatrick, C. F., Virani, S. S., Dixon, D. L., Ballantyne, C. M., & Remaley, A. T. (2024). Role of apolipoprotein B in the clinical management of cardiovascular risk in adults: An Expert Clinical Consensus from the National Lipid Association. Journal of clinical lipidology, 18(5), e647–e663. https://doi.org/10.1016/j.jacl.2024.08.013

Leave a comment